Chemotherapy is an essential and often life-saving part of cancer treatment. However, certain chemotherapy medications can sometimes affect the heart or blood vessels.
This possible effect is known as cardiotoxicity.
Not every chemotherapy patient will develop a heart problem. The level of risk depends on the medication, dose, treatment duration and the patient’s existing cardiovascular health.
Through cardio-oncology, patients can have their heart health assessed before treatment, monitored during treatment and followed after treatment when necessary.
At Cardiology Center Zacharias Kounnis, our cardio-oncology service in Cyprus provides personalised cardiovascular assessment for patients preparing for, receiving or recovering from cancer treatment.
Yes, some chemotherapy medications can affect the cardiovascular system. However, the risk is not the same for every patient or every cancer treatment.
Possible cardiovascular effects include:
Some effects may appear during treatment, while others may develop months or years later.
This does not mean chemotherapy should be avoided. Cancer treatment decisions must always balance the benefits of treating the cancer with the individual risk of side effects.
The purpose of cardio-oncology is to help patients receive effective cancer treatment while protecting their cardiovascular health as much as possible.
Cardiotoxicity is a general term for cardiovascular damage or complications associated with cancer treatment.
It may involve:
Cardiotoxicity is not always severe, and it does not always cause immediate symptoms.
In some patients, the first signs are only visible through an echocardiogram, blood test or other cardiovascular examination. This is why monitoring can be important even when the patient feels well.
Different chemotherapy medications may affect the cardiovascular system in different ways.
Anthracyclines are a group of chemotherapy medications that include:
These medications are used to treat several forms of cancer, including certain breast cancers, lymphomas, leukaemias and sarcomas.
In some patients, anthracyclines may damage heart-muscle cells and reduce the heart’s ability to pump blood effectively.
The risk may increase with:
Appropriate surveillance before, during and after anthracycline treatment can help identify cardiovascular changes before they progress to more serious heart dysfunction.
Fluoropyrimidines include medications such as:
These treatments may sometimes affect blood flow through the coronary arteries.
Possible symptoms can include:
Patients with existing coronary artery disease or several cardiovascular risk factors may require additional assessment.
Chest pain during chemotherapy should always be reported promptly to the medical team.
Cyclophosphamide is used in the treatment of several cancers and certain blood disorders.
Cardiovascular complications are uncommon at standard doses but may occur with high-dose treatment, particularly in patients with other risk factors.
Possible effects can involve:
Platinum-based medications include cisplatin and related treatments.
These therapies may sometimes affect blood vessels and increase the risk of:
The individual level of risk depends on the patient’s overall health, treatment plan and existing risk factors.
No. Not every patient receiving chemotherapy requires specialist cardio-oncology follow-up.
However, a cardiovascular assessment may be particularly useful if:
The goal is to identify which patients need closer monitoring rather than testing every patient in exactly the same way.
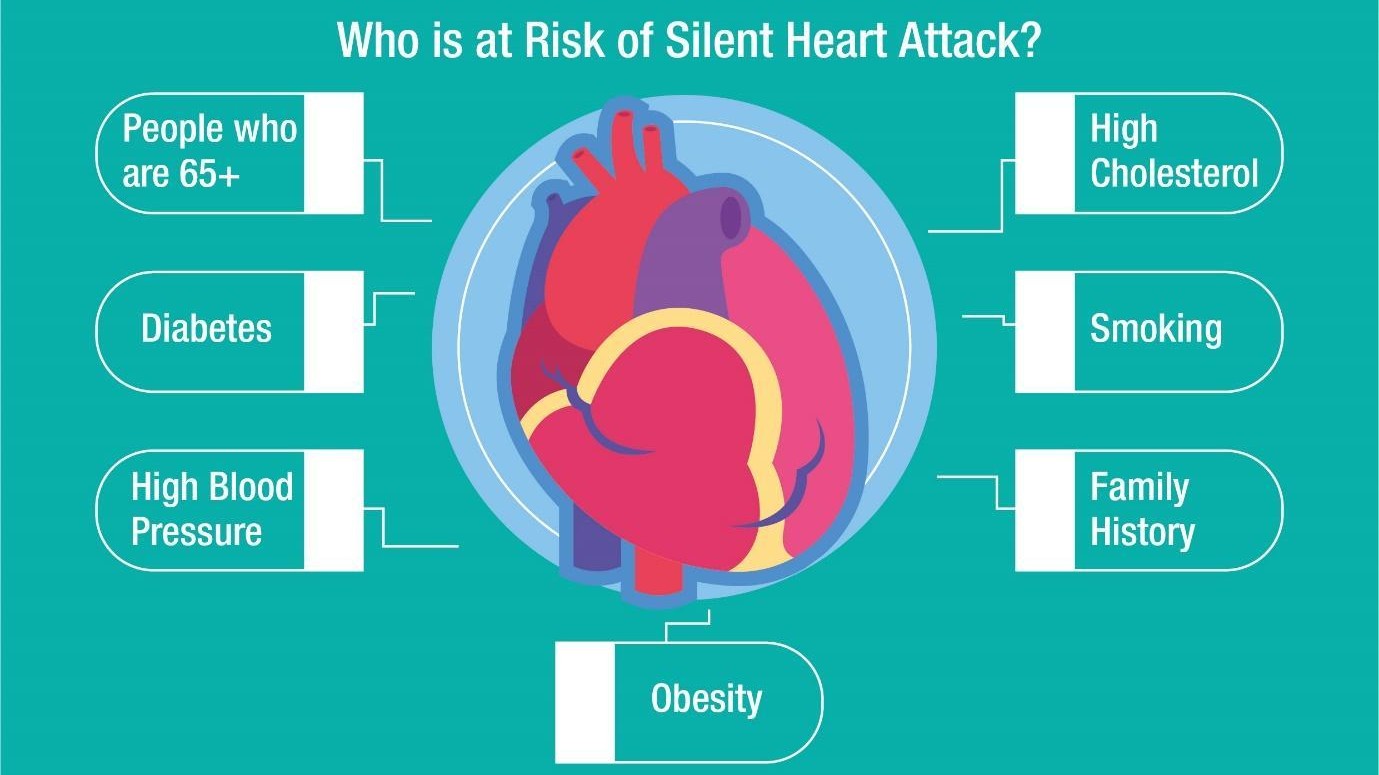
Several factors can increase cardiovascular risk during cancer treatment.
Patients with existing heart failure, coronary artery disease, cardiomyopathy or significant valve disease may be more vulnerable to additional cardiovascular strain.
Uncontrolled hypertension places additional pressure on the heart and blood vessels.
Managing blood pressure before and during chemotherapy can be an important part of reducing cardiovascular risk.
Diabetes can damage blood vessels and increase the risk of coronary artery disease and other cardiovascular complications.
High LDL cholesterol and other lipid abnormalities can contribute to the narrowing of arteries.
Depending on the patient, a cardiovascular assessment may include a standard lipid profile together with ApoB or Lipoprotein(a).
Previous exposure to anthracyclines or radiation involving the chest may affect future cardiovascular risk.
Your cardiologist should be informed about all previous cancer treatments, even if they occurred many years earlier.
Cardiovascular risk generally increases with age. However, younger patients may also require monitoring depending on the medication, dose and medical history.
Smoking damages blood vessels and increases the risk of heart attack, stroke and other cardiovascular complications.
Stopping smoking is one of the most important steps a patient can take to protect both cardiovascular and general health.
Possible warning signs include:
These symptoms do not always mean that chemotherapy has damaged the heart.
Cancer itself, anaemia, dehydration, infection, lung conditions, anxiety and other treatment side effects can cause similar symptoms.
However, new or worsening symptoms should be reported rather than ignored.
Severe chest pain, sudden breathing difficulty, fainting or rapidly worsening symptoms require urgent medical attention.
Yes.
Early changes in heart function may develop before the patient experiences breathlessness, swelling or other clear symptoms.
This is sometimes referred to as asymptomatic cardiac dysfunction.
Regular cardiovascular monitoring may detect:
Finding these changes early may allow the medical team to adjust monitoring, manage risk factors or begin cardiovascular treatment before more serious symptoms develop.
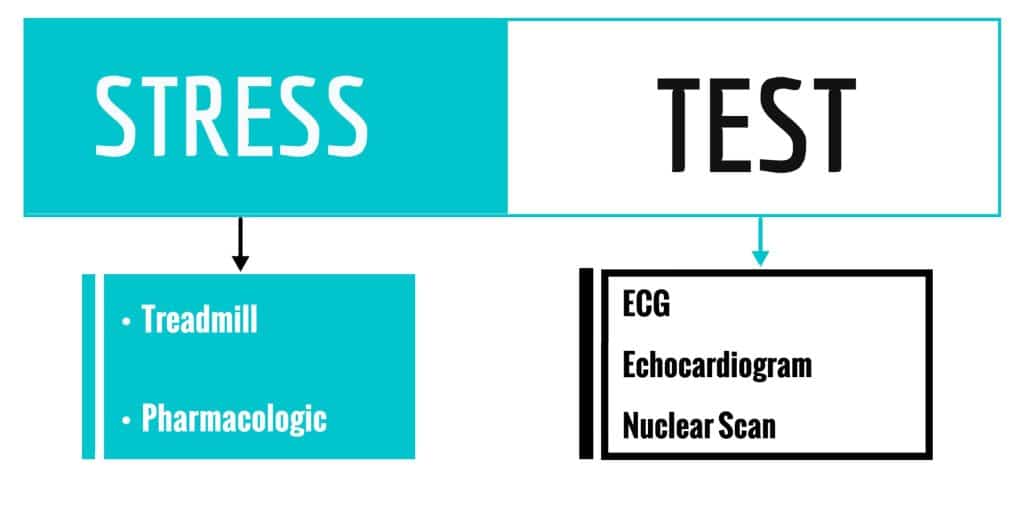
The tests recommended depend on the type of chemotherapy and the patient’s cardiovascular risk.
Not every patient needs every test.
An electrocardiogram, or ECG, records the electrical activity of the heart.
It may identify:
An ECG is quick, painless and non-invasive.
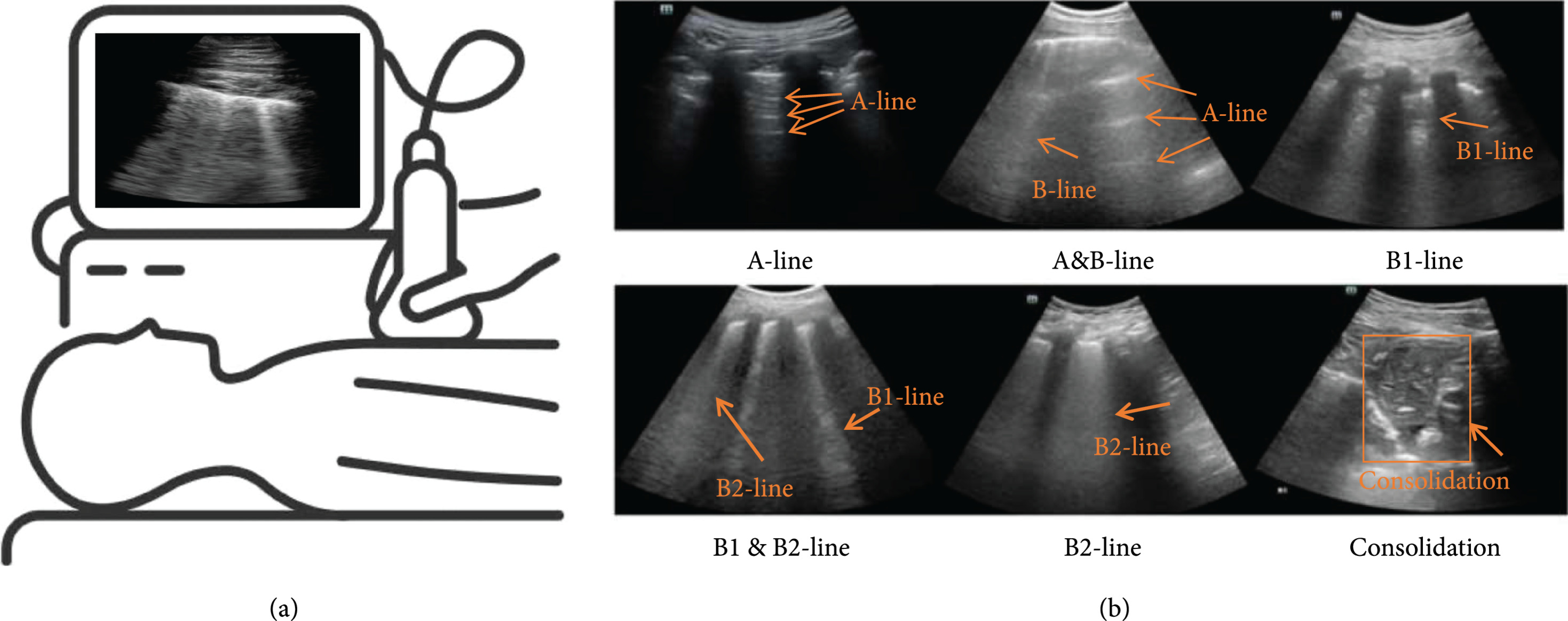
An echocardiogram uses ultrasound to examine the heart.
It provides information about:
A baseline echocardiogram can provide measurements that may be compared with future examinations.
Left ventricular ejection fraction, commonly called LVEF, estimates how much blood the left ventricle pumps out with each contraction.
It is an important measurement of heart-pumping function.
However, LVEF is only one part of a complete cardiovascular assessment. A patient may have early heart-muscle changes before a major reduction in ejection fraction becomes visible.
Global longitudinal strain, or GLS, is an advanced measurement obtained during an echocardiogram.
It assesses how the heart muscle shortens and contracts.
GLS may help identify subtle changes in heart function before they become obvious through standard measurements.
The results should be interpreted by an experienced cardiologist and compared with previous examinations whenever possible.
Selected patients may have blood tests that measure biomarkers associated with heart-muscle injury or strain.
These may include:
A single abnormal result does not automatically mean that chemotherapy has caused permanent heart damage.
Biomarker results must be interpreted together with symptoms, imaging findings, kidney function and the patient’s overall condition.
Some chemotherapy and other cancer treatments may increase blood pressure.
Monitoring may involve:
Consistently high readings should be discussed with the medical team.
Cardiac magnetic resonance imaging, or cardiac MRI, may occasionally be recommended when an echocardiogram does not provide enough information or when a more detailed assessment of the heart muscle is required.
It is not a routine test for every chemotherapy patient.
Whenever clinically appropriate, cardiovascular risk should be considered before potentially cardiotoxic cancer treatment begins.
A baseline assessment may include:
This creates a starting point for comparison during treatment.
A baseline assessment does not mean the patient already has heart disease. It helps the medical team understand the patient’s current cardiovascular health.
There is no single monitoring schedule for every patient.
The frequency depends on:
Some patients may only need a baseline evaluation.
Others may need repeat echocardiograms, ECGs, blood tests or blood-pressure checks during treatment.
The schedule should be personalised rather than based only on a fixed number of weeks or chemotherapy cycles.
It is not possible to prevent every cardiovascular complication. However, several strategies may help reduce risk.
A pre-treatment assessment can identify existing heart disease and risk factors that may need attention before chemotherapy begins.
Blood pressure should be measured and treated appropriately.
Patients who monitor their blood pressure at home should keep a record and report consistently high or unusually low readings.
Controlling cholesterol and blood sugar supports long-term cardiovascular health.
Medication decisions should be based on the patient’s individual risk and discussed with the treating doctors.
Smoking increases cardiovascular and cancer-related risks.
Patients who find it difficult to stop should ask their healthcare team about structured support.
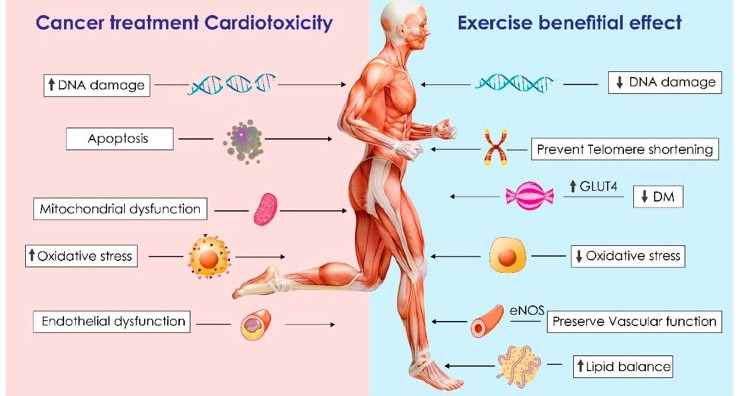
Appropriate physical activity can support cardiovascular fitness, muscle strength and general well-being.
The correct level of exercise depends on:
Patients should ask their oncology team before beginning a new or demanding exercise programme.
Patients with high blood pressure, heart disease, diabetes or high cholesterol should continue their medication unless their medical team advises otherwise.
Some patients at increased risk may be prescribed cardiovascular medication as part of a prevention or treatment plan.
These medicines are not automatically needed by every chemotherapy patient.
Do not wait until the next scheduled appointment to report significant chest pain, increasing breathlessness, fainting or rapidly worsening swelling.
Early evaluation may make complications easier to manage.
Finding a cardiovascular problem does not automatically mean that chemotherapy must be permanently stopped.
The cardiologist and oncologist may consider:
The decision depends on:
Communication between the oncology and cardiology teams is essential.
The aim is to protect the heart without unnecessarily compromising effective cancer care.
Some cardiovascular changes may improve, especially when they are detected and treated early.
The likelihood of improvement depends on:
Other complications may require longer-term monitoring or treatment.
This is one reason why patients should attend recommended follow-up appointments even when they feel well.
Some patients may need cardiovascular follow-up after chemotherapy has finished.
Follow-up may be particularly important if:
Depending on individual risk, follow-up may include an ECG, echocardiogram, blood tests or cardiovascular consultation.
Not every cancer survivor needs lifelong specialist monitoring. The follow-up plan should be based on treatment history and personal risk.
Where possible, bring:
Do not delay an appointment simply because some documents are unavailable. The assessment can begin using the information you have.
No.
Many patients complete chemotherapy without developing serious cardiovascular complications. The risk depends on the treatment, dose and individual health factors.
Monitoring is used to identify patients who may need additional protection or follow-up.
Do not stop chemotherapy on your own.
Report the palpitations to your oncology team. Depending on the symptoms, you may need an ECG, Holter monitor, blood tests or cardiovascular assessment.
Seek urgent help if palpitations occur with fainting, severe chest pain or serious breathing difficulty.
Yes.
A standard echocardiogram uses ultrasound rather than radiation. It is non-invasive and generally painless.
LVEF measures the percentage of blood pumped out of the left ventricle during each contraction.
GLS examines how the heart muscle itself shortens and contracts.
Together, these measurements can provide a more complete assessment of heart function.
Yes.
Some complications appear during treatment, while others may develop later. The level and duration of follow-up depend on the treatment received and the patient’s individual cardiovascular risk.
Many patients can benefit from appropriate physical activity, but the correct level varies.
Ask your oncology or cardio-oncology team before starting a new exercise programme, particularly if you have symptoms, low blood counts or an existing cardiovascular condition.
No.
Preventive cardiovascular medication may be appropriate for selected patients but is not automatically recommended for everyone.
The decision should be based on individual risk, medical history and test results.
Do not begin supplements without discussing them with your medical team.
Some supplements can interact with chemotherapy, cardiovascular medication or other treatments.
Chemotherapy can be essential for treating cancer, but cardiovascular health should also be considered as part of the complete treatment plan.
At Cardiology Center Zacharias Kounnis, our cardio-oncology service in Limassol provides personalised cardiovascular assessment for patients before, during and after cancer treatment.
Depending on your medical history and treatment plan, your evaluation may include:
Not every patient requires every test. The assessment is adapted to your cancer treatment, cardiovascular history and personal risk factors.
Concerns about heart health should not prevent patients from receiving necessary cancer treatment.
The best approach is informed, coordinated care.
A cardio-oncology assessment can help:
Early assessment provides the medical team with more information and more options.
Are you preparing to begin chemotherapy, currently receiving cancer treatment or concerned about your heart health after treatment?
Schedule a personalised cardio-oncology consultation at Cardiology Center Zacharias Kounnis in Limassol, Cyprus.
Our team can assess your cardiovascular risk, review your cancer-treatment plan and recommend appropriate monitoring before, during or after chemotherapy.
Book an appointment with our cardio-oncology service in Cyprus.
Medical disclaimer: This article provides general educational information and does not replace personalised advice from your oncologist, cardiologist or other healthcare professional. Never stop or change chemotherapy, cardiovascular medication or other prescribed treatment without medical guidance.

.jpg)

























.png)








.jpeg)



